WOMEN PHYSICIANS COLLECTIVE
The AI Gender Gap in Medicine Is a Problem Women Physicians Need to Help Solve
I think about AI in medicine more than almost anything else right now.
Specifically this: it is being built around us, used inside the systems we work in, and trained on data that has historically underrepresented us — while women physicians are adopting it at a lower rate than our male colleagues.
That combination is not a coincidence. And it's worth talking about directly.
Where Things Actually Stand
The AMA's most recent data shows cautious optimism growing alongside rapidly increasing AI usage among physicians. The Doximity 2026 State of AI in Medicine Report, which surveyed over 3,000 physicians across 15 specialties, found that daily AI usage jumped from 47% to 63% in a single year. 94% of physicians are now using or actively interested in AI.
The healthcare AI market is projected to hit somewhere between $45 and $51 billion in 2026 — and unlike a lot of projected numbers in healthcare, this one appears to have actually kept pace.
This is not a trend being discussed. This is infrastructure being built. Right now.
And here is the number we need to pay attention to: male physicians report 57% actual AI adoption. Women report 49%.
An 8-point gender gap in a technology that is actively reshaping how medicine is practiced. And we already know that women physicians spend more time in the EHR every day compared to male colleagues. The tool most likely to change that is the one we are adopting at a lower rate.
Why the Gap Matters More Than It Appears
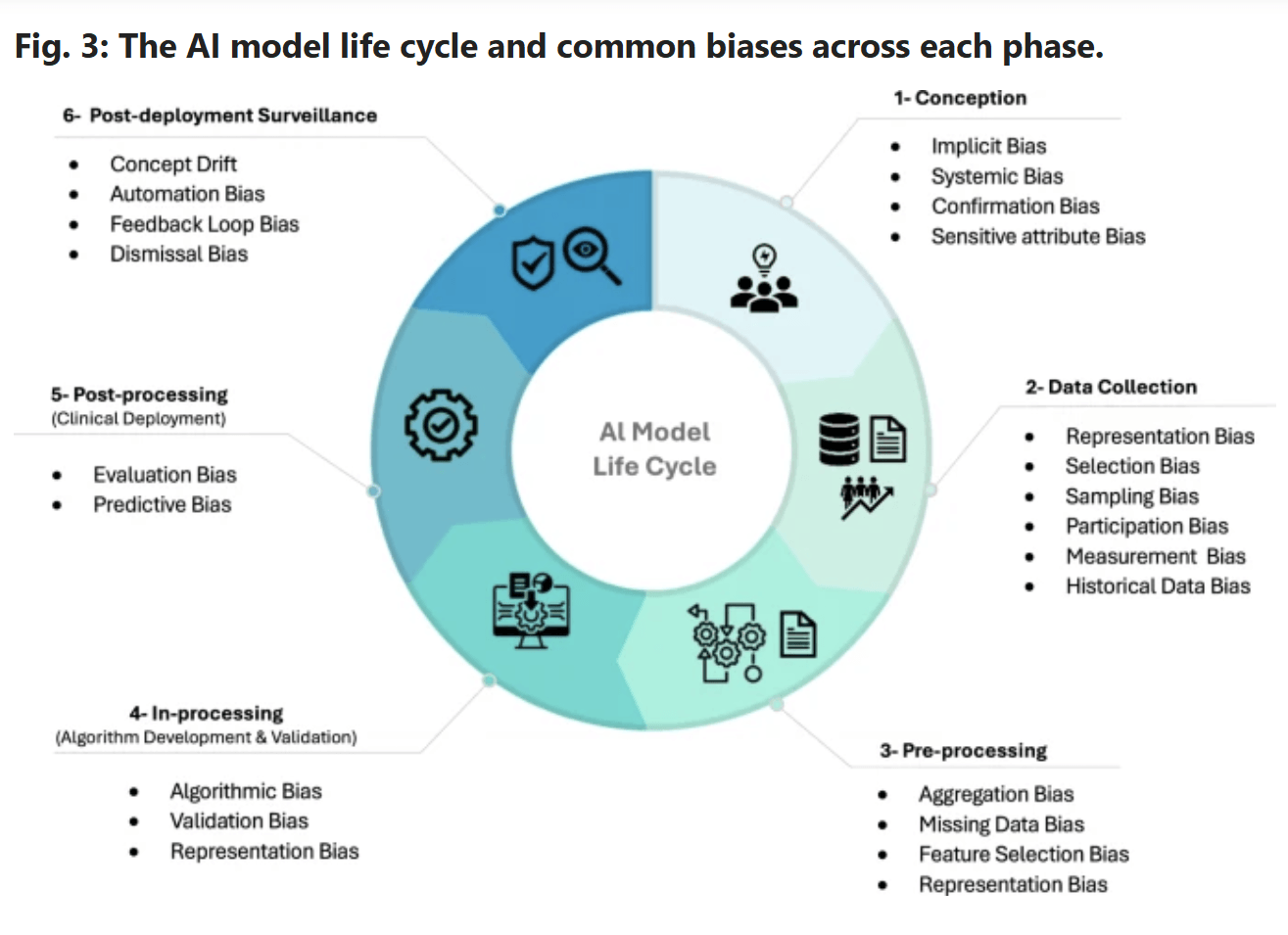
We already know AI has a bias problem. Research published in Science confirmed that AI vision-language models in medical imaging underdiagnose women. The disparities compound at the intersection of gender and race. The root cause is exactly what you would expect: training datasets that underrepresent these groups. This article in Nature's npj Digital Medicine examines bias in AI diagnostic tools with mitigation strategy suggestions. Figure 3 below:
The EU AI Act, now fully in effect, mandates representative training data for high-risk AI systems. The US has no equivalent standard.
So we have a technology being deployed at scale inside our hospitals, trained on data that skews away from women and women of color, with no federal mandate to fix it — and the physicians who could help improve this the most are the ones least represented at the table.
Women physicians are uniquely positioned to shape the future of healthcare AI. Not just as users of it. As the people who notice when it gets something wrong, who ask the questions nobody thought to ask, who bring the clinical perspective of half the physician workforce and a significant portion of the patient population.
But that only happens if we show up.
What AI Is Actually Doing for Documentation Right Now
Before we talk about what showing up looks like, let's talk about what is actually at stake — because the data on documentation time savings is not abstract.
JAMA recently reported the following from institutions that have implemented ambient AI documentation tools:
Emory Healthcare saw a 30.7% increase in documentation-related well-being after AI scribe implementation
Mass General Brigham reported a 21.2% reduction in burnout prevalence after 84 days of ambient documentation use
Cleveland Clinic physicians saved 14 minutes per day on EHR notes
Cooper University Healthcare saved over an hour of documentation time daily per physician
90% of physicians in the Doximity report said AI could reduce after-hours documentation. That is nearly universal agreement that this technology could give us back something we have been losing for years.
The physicians saving an hour a day on documentation were not tech early adopters. They were clinicians who tried something and found that it worked.
What Showing Up Actually Looks Like
It does not mean becoming a programmer or understanding how large language models are trained. It means using the tools, giving feedback on what is wrong, asking your institution how AI is being incorporated and how it was validated, and being willing to speak up when something doesn't look right.
Three things worth taking away from all of this:
1. The gender gap in AI adoption is a feedback loop. The less we use these tools, the less our experience informs how they are built. The less our experience informs how they are built, the more likely they are to underperform for our patients and for us. We have to pull up a chair to this table.
2. Your institution is almost certainly already using AI diagnostic tools. You are allowed to ask how AI is being incorporated into your systems and how it was validated. That is a completely reasonable clinical question, and it is yours to ask.
3. Starting is not as complicated as it feels. An AI scribe. A literature search tool. A single prompt that helps you draft a difficult patient letter faster. You do not have to overhaul your practice. You just have to start somewhere and notice what happens.
Why This Is a Literacy Issue, Not a Tech Issue
Understanding AI is now clinical literacy. The question is not whether AI is coming — it is already here. The question is whether we are passive recipients of a technology built largely without our input, or whether we become part of the conversation that shapes what it becomes.
Women physicians are seeing and treating the patients most likely to be harmed by a biased model. We have the clinical credibility and the daily clinical experience to push back on implementations that don't hold up. That voice matters. But it only lands if we are in the room.
Inside WPC, we are building out an AI playground where members can experiment with tools, ask questions, and think through the ethics and practical application of AI in medicine alongside other women physicians navigating the same questions. We are also offering a free AI primer workshop for women physicians — because this conversation deserves more than a think piece. It deserves a room.
In the meantime, if you want to stay current on research and resources like this, the newsletter, Notes from the Call Room, is where it lands first. Subscribe below.

I'm JMac.
I'm a pediatric hospitalist and the founder of Women Physicians Collective.
I started WPC because I've been alone in that call room, wondering who I was outside of being a doctor.
I write about the things nobody said out loud in medical school — identity, burnout, the weight women physicians carry, and what it actually takes to feel like yourself again inside this career.
This isn't a wellness blog.
It's a colleague who gets it, writing openly about the hard parts.
popular

Get on the list for the convos we don't get to have at work.
Weekly-ish drops on medicine and identity, women's health, community, AI, and the real tea about this wild ride.


©WOMEN PHYSICIANS COLLECTIVE LLC 2025 | SITE CREDIT | PRIVACY | TERMS & DISCLAIMERS